שיקום נשימתי ד"ר רונן בר-יוסף מכון ריאות ילדים מרפאת פעילות גופנית ותזונה נכונה בי"ח רות לילדים, רמב"ם
|
|
|
- Christopher Horace Stanley
- 5 years ago
- Views:
Transcription

1 שיקום נשימתי ד"ר רונן בר-יוסף מכון ריאות ילדים מרפאת פעילות גופנית ותזונה נכונה בי"ח רות לילדים, רמב"ם פברואר 2014 במסגרת "רפואת ספורט" - שנה א' SPORTS MEDICINE
2 DEFINITION Pulmonary rehabilitation is a comprehensive intervention based on a thorough patient assessment followed by patient-tailored therapies which include, but are not limited to, exercise training, education, and behavior change, designed to improve the physical and emotional condition of people with chronic respiratory disease and to promote the long-term adherence to health-enhancing behaviors
3 Pulmonary rehabilitation Entity on its own although combining different therapies These components are conveniently bundled into a package and delivered by professionals with expertise and experience Pulmonary rehabilitation is much more than the sum of its parts
4 Comprehensive intervention Pulmonary rehabilitation can be delivered at multiple times in the disease trajectory of any individual patient Its focus and components vary depending on the patient s goals, functional impairments, and disabilities Requires a dedicated interdisciplinary team, which may include: Physicians Nurses Nurse practitioners Respiratory therapists Physiotherapists Occupational therapists Psychologists, behaviorists Exercise physiologists Nutritionists Social workers
5 Thorough patient assessment To effectively treat the often complex and unique morbidities, these must be first identified Example: exercise limitation in a patient with COPD reflects multiple factors: Ventilatory constraints Ambulatory muscle dysfunction Cardiovascular limitation Joint disease Psychological and cognitive problems Identification will allow for a targeted and thereby more effective and efficient intervention
6 Patient-tailored therapies Intervention must be individualized to the unique therapeutic requirements of the patient, which result from the: Respiratory disease Comorbidities Treatments and their psychological and social consequences
7 Exercise training, education, and behavior change Exercise training and education aimed at behavior change are its essential components Exercise training remains the cornerstone of pulmonary rehabilitation, but it is not sufficient to provide optimal and long-term benefits Must be coupled with educational efforts aimed at promoting self-management skills and positive change in health behavior

8
9 הדרכה סרט -
10 Designed to improve the physical and emotional condition PR leads to substantial benefits in dyspnea, exercise capacity, health-related quality of life, and health care utilization These benefits other medical therapies such as bronchodilators, are achieved without improvement in traditional measures such as FEV 1 Paradox explained by the fact that rehabilitation targets the often treatable systemic manifestations of chronic respiratory disease: Peripheral muscle dysfunction Cardiovascular parameters Maladaptive health behaviors Anxiety and depression
11 Promote the long-term adherence to health enhancing behaviors 6-12 wk intervention such as exercise training can t have a substantial long-term impact on a chronic disease Need to include interventions that promote true health behavior change so as to maintain long-term benefits
12 Pulmonary rehabilitation Provide the right therapy for the right patient at the right time These therapies may include: Providing smoking cessation therapy Promoting regular exercise and physical activity in the home and community settings Fostering collaborative self-management strategies Optimizing pharmacotherapy and medication adherence Offering palliative care and hospice services
13
14 HISTORY - Early Years Components of pulmonary rehabilitation have been provided as part of good medical care for centuries In the 1960s s clinicians became aware that organizing these components into a comprehensive program could lead to substantial benefits for their patients Such components included breathing techniques, walking exercise, supplemental oxygen therapy, and bronchial hygiene techniques In 1974, pulmonary rehabilitation was first given an official definition by the American College of Chest Physicians In 1981 the American Thoracic Society published its first official statement on pulmonary rehabilitation
15 HISTORY - Early Years Development in 2 general outcome areas fueled the growing popularity of pulmonary rehabilitation among clinicians: 1) development of the timed walk test in ) Creation of the Chronic Respiratory Questionnaire, a patient-centered, health-related quality of life questionnaire for COPD, in 1987 Pulmonary rehabilitation led to often striking improvements in these outcome areas
16 Randomized Controlled Trials Demonstrating Global Benefit 1991 patients with COPD had a dose-dependent physiologic effect from exercise training Before this, conventional thought had been that these patients were ventilatory pump limited and could not achieve physiologic benefits from exercise training exertional dyspnea improved following pulmonary rehabilitation pulmonary rehabilitation resulted in improved health-related quality of life largest trial to date (N=119 subjects) compared with education alone, comprehensive pulmonary rehabilitation led to significant improvements in exercise tolerance, symptoms, and self-efficacy for walking COPD was a disease of the muscles and was therefore treatable by the exercise component of pulmonary rehabilitation trial of 200 patients with COPD in comparison with usual care, pulmonary rehabilitation not only improved the traditional outcomes of exercise capacity and quality of life but also reduced subsequent health care utilization
17 Acceptance as a Gold Standard of Care 2001 the Global Initiative for Obstructive Lung Disease (GOLD) endorsed pulmonary rehabilitation as a standard therapy for COPD In 2003 placed this intervention prominently in their treatment algorithm for stable COPD the National Emphysema Treatment Trial (NETT) incorporated pulmonary rehabilitation as required care for emphysema patients referred for lung-volume reduction surgery, and compared the surgical outcome against the gold standard, pulmonary rehabilitation
18 Funding as a Specific Entity in the United States by the Centers for Medicare and Medicaid Services 2010, the Centers for Medicare and Medicaid Services began funding pulmonary rehabilitation Although many pulmonary rehabilitation providers consider this funding to be insufficient to cover costs, it reflects acceptance of pulmonary rehabilitation by this important health care system in the United States


19

20

21

22

23
24 הערכה סרט -

25

26
27 Exercise Training in Pulmonary Rehabilitation
28 Observed in patients with COPD, interstitial lung disease and bronchiectasis, but not in individuals with asthma or cystic fibrosis

29
30 ENDURANCE EXERCISE TRAINING Definition: an activity in which large muscle groups are used continuously In the past, PR has focused primarily on aerobic endurance training 3 to 4 days/week, work-phase duration of min, progressively increasing up to min 6-8 weeks of endurance exercise training is thought to be the minimum time frame needed to achieve substantial effects Longer PR programs generally lead to more favorable results Main aim in COPD patients is to improve aerobic capacity and augment the ability to perform daily activities
31 ENDURANCE EXERCISE TRAINING Studies beneficial effects on peripheral muscle force, functional exercise capacity, peak work rate, and health-related quality of life Increased exercise capacity following PR can be attributed, in part, to centrally mediated improvements, such as reduced ventilatory requirement for a given task and increased peak aerobic capacity
32 ENDURANCE EXERCISE TRAINING Elicits improvements in structure of the lower-limb muscles: increased muscle fiber capillarization increased mitochondrial density increased oxidative capacity of muscle fibers delayed onset of the anaerobic metabolism Lower BODE index (COPD rating, including measures of BMI, airway obstruction, dyspnea, and 6MW) Because higher (worse) BODE scores predict mortality in COPD, this type of exercise intervention may improve mortality (never been confirmed prospectively)
33 ENDURANCE EXERCISE TRAINING Supervision of a health care professional such as a physiotherapist or exercise physiologist, is highly recommended Target training intensity is usually monitored by work rate and perceived exertion Exercise training at 60-90% of peak work rate is usually defined as high-intensity exercise superior to lower intensity training in achieving physiologic improvements in aerobic exercise capacity An intensity > 60% of the peak work rate can usually be sustained for short periods only, ranging from 4-10 min in patients with moderate-severe COPD <20% of patients sustain this continuous high-intensity exercise throughout the PR program Low-intensity to moderate-intensity continuous training (50% to 60% of peak work rate or a score of 5 to 6 points on the modified Borg scale) can also lead to gains in exercise endurance, even in patients with advanced disease


34
35 INTERVAL EXERCISE TRAINING Definition: repeated short periods of exercise alternated with rest Duration of the work interval and the recovery interval can vary greatly and depend on the duration of the work phase In healthy individuals the metabolic changes, including cardiorespiratory responses and low muscle lactate concentrations, during interval exercise are similar to those of continuous moderate exercise Interval training is an attractive alternative to continuous training, especially in those patients with COPD who develop severe dyspnea during exercise Intermittent recovery periods during interval training decrease in endexpiratory lung volume and prevent high lactate accumulation, which results in lower ventilation and less dyspnea
36 INTERVAL EXERCISE TRAINING Compared with continuous high-intensity training, interval training results in fewer unintended breaks (decreased ventilatory requirement?) Deliver an adequate load to the exercising muscles, resulting in the desired peripheral adaptations with less dyspnea burden In COPD beneficial effects, equivalent to those of continuous training in terms of exercise capacity and health-related quality of life Interval protocols with varying work phases, passive or active recovery significant training effects
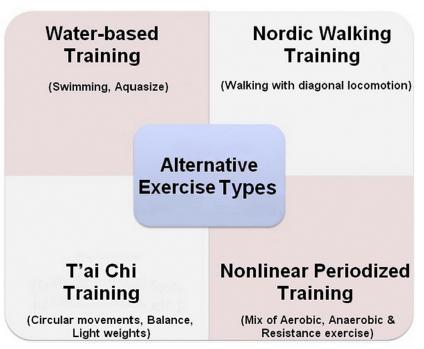
37 RESISTANCE TRAINING Muscle strength is important for optimal health, functional performance, and quality of life The expected loss of muscle mass and strength with age can progress more slowly when elderly individuals participate in resistance exercise training programs Fundamental principles of resistance training are: Progressive overload Variation Specificity The intervention must be tailored to the specific needs of the individual to maximize outcomes Accomplished by the incorporation and manipulation of the following variables: Intensity Volume (=number of sets and repetitions) Training frequency Rest interval between sets Sequence of exercises Movement velocity
38 RESISTANCE TRAINING Intensity is considered the most important variable, and is inversely related to the training volume Studies in healthy elderly subjects show that resistance training also improves skeletal muscle oxidative capacity and endurance, and increases capillarization and oxygen flux through the skeletal muscle Before 1990, resistance training was not recommended for rehabilitative exercise
39 RESISTANCE TRAINING In COPD, resistance training is an ideal intervention for those patients who have peripheral muscle weakness and intensive symptoms of dyspnea during physical activity or exercise Daily activities such as maintaining balance while standing, rising from a chair, or lifting objects constitute a challenge It is assumed that resistance exercise training can partially reverse peripheral muscle weakness and thus reduce this aspect of the systemic burden of COPD Upper and lower extremity resistance + aerobic training = improvements in: Strength lean body mass functional exercise capacity 3 of 8 simulated activity of daily living tasks compared with aerobic training alone
40 RESISTANCE TRAINING Patients with COPD who underwent resistance exercise training program showed increased improvements in quality of life ATS/ERS statement on PR (2013) should be performed At moderate intensity (50% 85% of the RM1) Include 2-4 sets of 6-12 repetitions 2-3 times a week Several studies in patients with COPD, using similar approaches showed increased peripheral muscle strength
41 פעילות סרט -
42 GROUND WALKING EXERCISE TRAINING Treadmill walking and stationary cycle training have traditionally been the prominent exercise training modalities in comprehensive PR A home based unsupervised walking program, 6 days per week for 12 weeks, in patients with COPD almost doubled endurance walk time compared with a control group Study ground walking vs. stationary cycle training in patients with COPD: Improved endurance walking capacity to a greater degree As effective in: Improving peak walking capacity Peak and endurance cycle capacity Quality of life
43 GROUND WALKING EXERCISE TRAINING Recommended intensity is: 80% of the average speed on the 6MW test 75% of peak speed attained with moderate dyspnea sensation (3 on the modified Borg scale during the incremental shuttle walking test)
44 NORDIC WALKING EXERCISE TRAINING Developed as an off-season training method for competitive cross-country skiers Europe s fastest growing form of exercise Diagonal locomotion using longer steps Requires coordinated movements for balance and stability, strength and endurance, varied cardiovascular efforts, agility, and visual acuity
45 NORDIC WALKING EXERCISE TRAINING In healthy individuals: More intense workout than normal walking at the same speed Higher peak heart rate Higher oxygen consumption (even compared with jogging) Recommended as an effective and efficient mode of exercise to improve overall functional fitness in elderly people Additional benefits in functional capacity and muscular strength compared with regular walking, and is suitable for improving endurance in elderly adults
46 NORDIC WALKING EXERCISE TRAINING Positive effects in people with chronic diseases: Improved mobility in patients with Parkinson disease Increased exercise capacity in men after acute coronary syndrome Enhanced quality of life in overweight individuals with diabetes Nordic walking is safe, feasible, and effective in patients with COPD Compared with usual care, a supervised, 3-month, outdoor Nordic walking exercise program at 75% of initial maximum HR, 3 times/wk for 1 hour/session increased exercise tolerance and daily physical activity (walking time and intensity) The observed improvements in exercise capacity and physical activity remained up to 6 months after completion of the intervention
47 WATER-BASED (OR AQUATIC) EXERCISE TRAINING Lower extremity exercise in a low-impact, resistance based environment, and uses similar training principles to land-based training Gain all the advantages of land based exercise + buoyancy of water facilitates balance and gait without overt stress or strain on arthritic joints Walking, cycling, and lifting weight, can be performed in a swimming pool Suggested water temperatures vary from 29 C -38 C Improvements in exercise performance, muscle strength, and balance in the elderly with and without chronic conditions
48 WATER-BASED (OR AQUATIC) EXERCISE TRAINING - in COPD Suggested as a new therapeutic training modality in patients with COPD Improving exercise capacity and quality of life Can be an alternative training approach to traditional land-based exercise programs Land-based programs are difficult for patients + coexisting obesity, musculoskeletal, or neurologic limitations BUT requires adequate duration and frequency in order to provide important benefits to patients with COPD Recent study found that a single, weekly maintenance water-based exercise session program did not maintain the improvements in physical activity and quality of life that had resulted from 3 sessions per week on a high-intensity, 3-month water based training program
49 WATER-BASED (OR AQUATIC) EXERCISE TRAINING - in COPD Additional beneficial physiologic effect caused by the hydrostatic pressure The hydrostatic pressure exerted during immersion can facilitate expiration and thereby reduce the degree of air trapping Vital capacity decreases up to 10% Functional residual capacity reduces to about 54%, Expiratory reserve volume decreases by 75%
50 TAI CHI Includes gentle circular movements, balance exercise, weight lifting, breathing techniques, and mental concentration Traditional tai chi includes various movements that are performed in a slow, relaxed manner for 30 minutes There are many styles of tai chi and each style has its own form The most popular and widely practiced style of tai chi is the Yang style, which includes 24 movements in its simple form and 108 movements in its traditional form Frequency and duration that may result in beneficial effects varies from 1-3 times per week for 4-16 weeks, with individual sessions lasting 45 to 60 minutes However, the recommended intensity is 50% to 58% of heart rate reserve for people from 25 to 80 years old
51 TAI CHI Long-term regular tai chi exercise training has beneficial effects on balance, flexibility, muscular strength, cardiovascular fitness, cognition, sleep quality, and emotional functioning in elderly adults Furthermore, Tai chi also has beneficial effects in individuals with mild hypertension, stroke, fibromyalgia, rheumatoid arthritis, knee osteoarthritis, diabetes, Parkinson disease and other chronic diseases Limited data suggest that tai chi may be beneficial in patients with COPD Meta-analysis of 8 randomized controlled trials, tai chi improved exercise capacity, dyspnea, quality of life, and lung function compared with general exercise or usual care in COPD
52 NLPE Nonlinear Periodized Training Traditional exercise training during PR uses a non varied, linearprogressive protocol orderly increase in exercise stress (intensity and duration) is placed on the body Traditional session usually consists of a combination of endurance + resistance training with both the aerobic and anaerobic systems providing the necessary energy for muscular contractions Athletes use nonlinear training methods directed to specific individual training goals NLPE is a training strategy that is designed to: Maximize individual adaptation Prevent overtraining Attain an optimal training effect by frequent variation in number of exercises, training intensity, exercise duration, and resting periods
53 NLPE Nonlinear Periodized Exercise To optimize physiologic adaptation aerobic and anaerobic energy systems are preferentially stimulated and matched during endurance and resistance exercise within 1 training session Variation in low-intensity and high intensity exercise interspersed with adequate recovery has been shown to be important for healthy adults suggested to result in a more fatigue resistant fiber type Applying principles of nonlinear exercise training in athletes to patients with severe to very severe COPD is feasible and worthwhile 10-week NLPE program (3 sessions per week) was superior in improving cycle endurance and health-related quality of life compared with traditional non varied exercise training The Future?

54

55


56

57
58
59

60
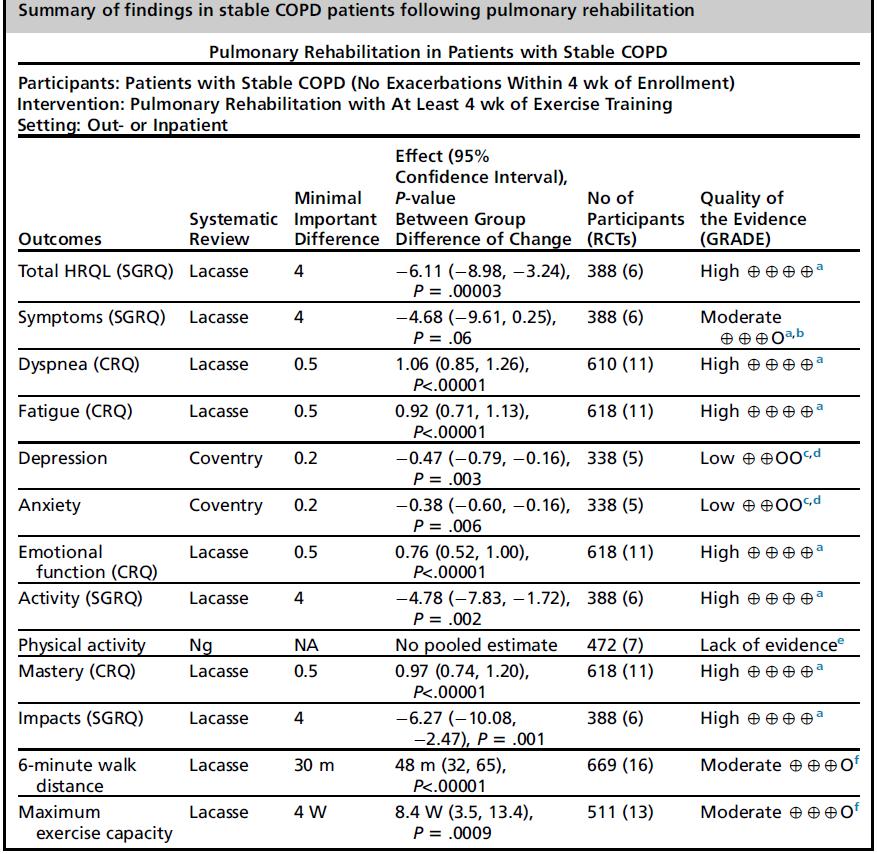
61 Activity and Exercise Capacity Challenge that occurs when both objective and subjective measures are included Activity following PR measured by activity monitors or physical activity questionnaires has not, to date, been sufficiently evaluated Recent meta-analysis of physical activity one could not adequately evaluate activity due to the variation in measures of activity (activity monitors, questionnaires) and lack of established minimal important difference (MID) Moderate quality of evidence (downgraded because of risk of bias) that PR has a strong effect on exercise capacity as measured by the 6-minute walk distance (6MWD) or maximum exercise capacity
62

63
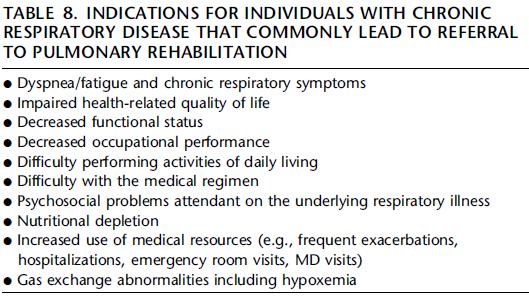
64 RATIONALE FOR PR IN NON-COPD DISORDERS The scientific rationale for PR for persons with COPD is that it can stabilize or reverse many systemic manifestations of the disease, including skeletal muscle dysfunction Participation in PR also improves: Exercise capacity Reduces knowledge deficits Promotes use of long-term health-enhancing behaviors Reduces depression and anxiety Helps patients manage complex medical regimens and exacerbations Reduces hospitalizations Improves patients QOL Can improve physical activity levels
65 RATIONALE FOR PR IN NON-COPD DISORDERS In many disorders (ILD, CF, pulmonary hypertension (PH), and lung cancer) low exercise capacity is associated with worse survival Improvement in exercise capacity via participation in PR has the potential to improve long-term outcomes of the disease
66 Recommended formally in both the 2013 ATS/ERS joint American College of Chest Physicians/American Association of Cardiovascular and Pulmonary Rehabilitation evidence-based guidelines Retrospective non-copd respiratory disorders achieve similar improvements in exercise tolerance, symptoms, and QOL after PR to those achieved by persons with COPD

67 Asthma Asthma affects all age groups and is a leading cause of chronic illness in children and adults
68 Asthma Airflow obstruction, increased work of breathing and symptom exacerbation (EIB) dyspnea, less tolerance for exercise despite optimized pharmacologic therapy low physical activity levels Poor asthma control is associated with a greater prevalence of functional impairment, depression, sleep disturbances, and reduction in daily activities Lower fitness and physical activity levels are associated with decreased ability to perform ADLs, increased psychological distress, impaired QOL and increased risk of asthma exacerbations Many studies have reported benefits of exercise training for patients with asthma
69 Asthma Review of RCTs examined 16 studies involving 516 patients between 6-18 years with asthma of varying severity Aerobic capacity (VO 2 max) improved after exercise training QOL: Cochrane 2012, 19 randomized studies (695 participants) including patients > 8 years with diagnosed asthma, physical training 20 minutes, 2 times/wk, over a minimum period of 4 wks Improved VO 2 max and maximum ventilation significantly Training was well tolerated None of the studies reported worsening of asthma symptoms or adverse effects with training Several studies also reported statistically and clinically significant improvements in health-related QOL
70 Asthma Adults: Improvements in cardiovascular conditioning (as measured by VO 2 max and decreased maximal exercise heart rate [HR] and minute ventilation) A longer walk distance as measured by the 6MWT or 12-minute walk tests Improved symptoms Improvement in QOL scores Less fear of experiencing breathlessness during exercise Less anxiety about exercising at high intensities
71 Asthma Exercise training program recommended for adult patients should include both physical and breathing exercise CPET should be considered before beginning training to assess patients for EIB Warm-up and cool-down periods should be provided routinely to minimize the risk of EIB during training Patients should use their inhaled bronchodilator before exercise training sessions

72 Cystic Fibrosis (CF) CF is an AR disease characterized by impaired chloride secretion, resulting in excessively thick bronchial secretions, altered respiratory mechanics, gas exchange, and pancreatic insufficiency Current median predicted survival age for patients with CF has increased steadily from age 31.3 years in 2002 to age 41.1 years as of 2012
73 CF Persons with CF have impaired exercise capacity and low physical activity levels Why? Decreased pulmonary function Gas exchange Cardiocirculatory disturbances EIB Skeletal muscle weakness Altered expression of the CF transmembrane regulator in muscle contributes to altered exercise energy metabolism and may contribute to skeletal muscle dysfunction High metabolic demands (increased effort of ventilation) vs low metabolic income (pancreatic insufficiency) nutritional impairment skeletal muscle wasting, reduced bone density, and impaired QOL
74 CF Several RCTs + uncontrolled trials exercise training can improve exercise capacity or muscle strength, regardless of disease severity, for both children and adults Significant improvements in peak aerobic capacity and QOL Resistance training significantly fat free mass, and leg strength Inspiratory muscle training can also improve respiratory muscle strength, pulmonary function, and exercise tolerance Respiratory muscle strength can also improve through moderate vigorous aerobic exercise
75 CF Exercise rehabilitation: Habitual physical activity QOL Mechanical impedance of sputum optimization of airway clearance Goals: improving exercise tolerance and physical activity levels, optimizing functional capacity, increasing upper and lower body strength, optimizing bronchial hygiene, and reducing the rate of disease progression A combination of aerobic and resistive exercise training and flexibility exercises should ideally be incorporated
76 CF Supplemental oxygen, should be titrated to maintain oxygen saturations 88-90% during exercise Adequate hydration (excessive salt excretion and fluid loss during activity) Beware: CF-related diabetes and osteoporosis when creating an exercise plan Prevent cross contamination and the spread of resistant organisms, strict hygiene standards, infection control measures, and isolation precautions are essential

77 Non-CF Diffuse Bronchiectasis Characterized by persistent cough, excessive sputum production, and recurrent chest infections Chronic airflow obstruction may be present, and intermittent acute exacerbations of symptoms and bronchoconstriction often occur Similarities between COPD and bronchiectasis primary pulmonary involvement and secondary peripheral muscle, as well as nutritional and health-related QOL impairments
78 Non-CF Diffuse Bronchiectasis Prospective RCT 8 weeks of high-intensity exercise training consisting of 45 minutes of aerobic activity ± inspiratory muscle training vs. standard medical care significant improvements in exercise capacity, but benefits in health-related QOL were reported only with the combination of inspiratory muscle training and PR Retrospective studies: exercise tolerance and health status and may improve some aspects of pulmonary function (VC and RV) PR strategies for patients with non-cf bronchiectasis are similar to those recommended for patients with COPD and persons with CF
79 PR FOR RESTRICTIVE PHYSIOLOGY ILD/Pulmonary Fibrosis ILD (diffuse parenchymal lung disease) is a heterogeneous group of disorders in which the lung interstitium and/or alveolar spaces are involved with varying degrees of inflammation or fibrosis Typical symptoms of ILD include: Disabling exertional dyspnea Nonproductive cough Fatigue Other symptoms may also be present when the ILD is part of a systemic disease Patients with ILD have reduced exercise tolerance and low physical activity levels and experience depression and impaired QOL Exercise limitation in ILD has a multifactorial basis including ventilatory, cardiocirculatory, and gas exchange derangements Resting pulmonary function testing does not reliably predict exercise limitation in ILD Exercise-induced hypoxemia is often profound
80 ILD/Pulmonary fibrosis Skeletal muscle dysfunction can contribute to exercise impairment Study of 12 persons with ILD, the symptom of leg fatigue was the principal cause of cessation of exercise in 17% and led to cessation of exercise together with the symptom of dyspnea in 58% of patients Quadriceps force correlates to: The symptom of leg fatigue during exercise VO2max 6MWD Depression Low exercise tolerance is associated with worse QOL and lower survival
81 PR for RESTRICTIVE PHYSIOLOGY ILD/Pulmonary fibrosis Limited pharmacologic treatment options are available for many PR is a recommended as a component of care in the ATS/ERS guidelines on IPF and is typically required of patients before they undergo lung transplantation
82 Several studies have demonstrated that patients with ILD can benefit from PR Most of the studies small cohort studies 2 RCTs are available In most of the studies PR has led to significant improvements in 6MWD, post-pr improvements in dyspnea, and improvements in QOL Less in IPF PR programs have been outpatient programs of 8-12 weeks duration, in which patients underwent supervised multimodality aerobic and strength training of the lower and upper extremities as well as participated in an education program (recommended) The optimal content and duration of the exercise training regimen for patients with ILD remains uncertain
83 ILD/IPF Patients should be assessed for comorbidities their supplemental O2 requirements before and during PR, and SaO2 should be kept greater than 88-90% during exercise when possible High FiO2 up to 100% (or high flow) may be required to maintain adequate oxygenation during exercise
84 Restrictive Chest Wall Disease Chest wall deformities such as scoliosis and kyphosis are common in both pediatric and adult populations Impairments include: Abnormal pulmonary function (restrictive physiology ) Gas exchange disturbances (principally related to hypoventilation) Cardiovascular alterations Symptoms of dyspnea on exertion, cough, easy fatigability, pain in the anterior chest, tachycardia, and chronic mucus expectoration Elderly people + hyperkyphosis physical deconditioning and are at increased risk of falls, earlier mortality
85 Restrictive Chest Wall Disease Treatments include: Respiratory exercise therapy General physical conditioning Muscle and spinal exercise-based interventions Pharmacotherapy to delay progression of kyphosis Spinal orthotics and postural taping Surgical interventions
86 Restrictive Chest Wall Disease Review: effectiveness of exercise training in treating adolescent patients with scoliosis exercise didn t conclusively prevent the progression of spinal curvature General strength Neuromotor control Stability of the spine Breathing function and postural balance improved 2 more studies also showed that 8-12 weeks of aerobic exercise training, including treadmill walking, arm ergometry, and bicycling, improvements in 6MWT and lung function
87 PR in Pulmonary Hypertension (PHT) Arises from a wide variety of conditions Pharmacologic therapies have led to improved clinical outcomes Principal symptoms include: Exertional dyspnea Exercise/activity intolerance Atypical chest pain Palpitations Dizziness Fatigue
88 PHT Exercise capacity is impaired among persons with PH as a result of multiple factors: Pulmonary function Gas exchange Cardiocirculatory impairments Skeletal muscle dysfunction Low exercise capacity in persons with PAH is associated with worse clinical outcomes Peak VO2 of 10.4 ml/min/kg17 or less and 6MWD less than 332 m have been associated with worse survival PAH symptoms of fatigue, anxiety, and depression may have cognitive impairment and report impaired QOL
89 PHT Several studies PR and exercise training administered carefully are safe, well tolerated, and can improve several of these clinical outcomes Supplemental oxygen to avoid desaturations less than 88-90% Intensity of exercise was limited to 60-80% of maximal HR identified during pretraining CPET or to 70-80% of HR reserve No serious adverse events occurred as a consequence of rehabilitation in most of these studies Transient dizziness (without syncope) was reported by a few patients No formal guidelines for exercise training and rehabilitation yet exist for patients with PH

90 PR for PHT
91 Lung Cancer Strong rationale for providing PR to patients with lung cancer Lung cancer is present concurrently with COPD May also complicate other forms of chronic respiratory disease Poor overall survival Low exercise tolerance is associated with: Worse surgical outcomes after resection of malignancy Worse responses to chemotherapy (in terms of toxicity and disease progression-free intervals) Reduced survival
92 Low exercise tolerance (eg, VO 2 max < 15 ml/kg/ min, 6MWD < 61 m [200 ft], or inability to climb a flight of stairs) greater risk of postoperative pulmonary complications after lung resection surgery May be used to exclude patients from undergoing lung resection surgery PR has the potential to improve exercise capacity Patients considered inoperable may become candidates for potentially curative surgical treatment Those with relatively low performance status may become candidates for chemotherapy
93 Lung cancer Several studies have documented clinical benefits of PR Preoperative PR before lung cancer resection surgery can lead to improved exercise endurance (6MWD or cycling endurance), increased VO 2 max and improved muscle strength Postoperative PR has also led to improvements in exercise endurance, strength, peak work rate and reduced dyspnea Some trials improvement in QOL The type, intensity, and duration of exercise training should be guided by the clinical circumstances
94 PR Before Lung Transplantation PR plays a vital role when managing lung transplant patients preoperatively There are no formal guidelines regarding the content of pretransplant PR PR improves functional outcomes, including the 6MWT and QOL Recent study supports that every 100-m increase in 6MWD correlates with a 2.6-day decrease in median hospital length of stay Preoperative PR may also reduce the risk of postoperative complications,
95 PR After Lung Transplantation Regardless of the underlying diagnosis or lung disease before transplant, and despite near normalization in lung function after transplant activity intolerance often persists for years 50% of predicted exercise capacity 30 month postoperatively Skeletal muscle weakness and dysfunction deconditioning immobilization during hospitalization + glucocorticoid therapy + immunosuppressive medications Post transplantation PR can significantly improve quadriceps force, functional capacity, and QOL

96
97
98 Regular physical activity is of critical importance in long-term prognosis Exercise and physical activity are not identical concepts Physical activity comprises any bodily movement produced by skeletal muscles that results in energy expenditure Exercise is a subset of physical activity that is planned, structured, repetitive, and purposeful Improvements in exercise capacity (after a PR) do not necessarily result in improvements in daily physical activity in the home and community settings

99 HOW PHYSICAL ACTIVITY IS MEASURED AS AN OUTCOME OF PULMONARY REHABILITATION
100 Energy-expenditure assessment Aims at measuring how much energy is spent in physical activity, and not specifically at measuring the amount and intensity of the physical activity performed Energy expended in physical activity depends on several factors such as age, gender, body mass, movement efficiency, and the energy cost of each activity This complexity, along with difficulties in measurement and high cost hinders the use of energy expenditure assessment in clinical practice or even in scientific studies Leaving questionnaires and motion sensors as the most frequently used methods to measure physical activity
101 Questionnaires Aim at capturing different aspects of physical activity, such as amount, type, intensity, symptom experience, and performance of activities of daily living Questionnaires are easy to use and inexpensive
102 Motion sensors Devices that detect body movement, and therefore can be used to objectively quantify physical activity in daily life for periods of time Small, light, and minimally intrusive Main types of motion sensors are: Pedometers - count the number of steps performed by the subject, Accelerometers - detect body acceleration, capable of estimating time spent in activity, energy expenditure, and a variety of other outcomes related to physical activity in daily life Some motion sensors combine movement data (accelerometers) with physiologic data (heart rate and skin temperature sensors)
103 Motion sensors Recent studies few instruments that seem to be superior to others when assessing physical activity: DynaPort Mini Mod (McRoberts, The Hague, the Netherlands) ActiGraph GT3X (ActiGraph, Pensacola, FL) Sense- Wear Armband (SMT Medical, Wu rzburg, Germany) (all triaxial accelerometers), Which were found to be valid and responsive for use in COPD in the context of pulmonary rehabilitation
104 EFFECTS OF PULMONARY REHABILITATION ON PHYSICAL ACTIVITY Physical activity has only been recently included as an outcome of pulmonary rehabilitation Most studies patients with COPD Inconsistent results: some have demonstrated statistically significant increases in activity level after pulmonary rehabilitation, whereas others have not An overall interpretation of these results is difficult because of differences in the type of patients, content of programs, duration of programs, and methods for assessing physical activity Some of the studies had no control group or had a control group without random allocation and many had a small sample size
105 The well-documented and consistent benefit on exercise capacity lack of clear cut and consistent effects on physical activity Why? First exercise capacity is a functional status whereas physical activity is in large part a behavior Some recent PR incorporating behavioral components, such as feedback by pedometer or group activities, have shown positive effects on physical activity Second relatively short duration of many PR programs probably too brief to prompt the effective behavior changes required to increase physical activity in the home and community settings
106 CHALLENGES OF PULMONARY REHABILITATION IN PROMOTING PHYSICAL ACTIVITY Increase (or maintenance) of daily physical activity up to the recommended level (30 min/day of moderate physical activity on most days of the week) Should be a target of PR programs This goal irrespective of the underlying disease or baseline levels of physical activity

107
108 SUPPLEMENTAL OXYGEN Exercise-induced oxyhemoglobin desaturation is common in PR participants 572 people with COPD undertaking a 6MWT desaturation of 4% or greater to less than 90% occurred in 47% of tests No strong data regarding the adverse effects of transient oxyhemoglobin desaturation during exercise Supplemental oxygen improves exercise performance and reduces dyspnea in people with COPD Related to a reduction in ventilation for a given exercise workload, leading to a delay in dynamic hyperinflation and prolonged exercise time
109 Rationale These effects have been shown both in desaturators and nondesaturators Reduction in ventilation associated with a slower increase in blood lactate as a result of better oxygen delivery to peripheral muscle or direct chemoreceptor inhibition Supplemental oxygen may facilitate training of the muscles at a higher intensity, or for a longer duration, to enhance training benefits BUT..

110
111 Cochrane review small effects of supplemental oxygen during training on: Endurance time at the end of the program (2.69 min > room air Borg dyspnea score at the end of the endurance test (mean reduction of 1.22 points) No data to support effects on health-related quality of life or longer term clinical outcomes
112 Recent guidelines for PR reflect both the uncertainty arising from this body of literature and the common use of supplemental oxygen in clinical practice: BTS guidelines supplemental oxygen should not be used routinely, but should be offered to those who fulfill the criteria for long-term oxygen therapy or ambulatory oxygen therapy ATS/ERS statement individualized oxygen titration trials should be used to identify those people with COPD who may respond to oxygen supplementation during exercise testing Conclusion a trial of supplemental oxygen may be justified in both desaturators and nondesaturators if dynamic hyperinflation or severe dyspnea limit the progression of exercise intensity or duration
113 WATER-BASED EXERCISE High prevalence of comorbid conditions in people who have been referred to a PR program Three RCTs have compared the effects of land-based exercise, water-based exercise, and a control group: Endurance shuttle walk test Exercise capacity, measured via the 6MWT No serious adverse events and high levels of acceptability as an alternative training Good effect on joints + hydrostatic force on the chest wall associated with water immersion may assist in reducing lung volumes during exercise
114 INSPIRATORY MUSCLE TRAINING In people with COPD, pulmonary hyperinflation serves to shorten and flatten the diaphragm, reducing its mechanical advantage and pressuregenerating capacity This reduction in pressure-generating capacity has been associated with the severity of dyspnea and also with impairments in exercise capacity Traditional exercise training, such as walking and cycling, does not impose sufficient load on the inspiratory muscles to induce a training adaptation Specifically loading the inspiratory muscles, with the goal of improving their function as a way to ameliorate dyspnea and optimize exercise tolerance RCTs have examined the effects of IMT applied in isolation and combined with exercise training
115 INSPIRATORY MUSCLE TRAINING Meta-analyses of these trials provide strong evidence that IMT improves inspiratory muscle function (strength and endurance) and reduces dyspnea There is some evidence that IMT improves exercise capacity and health-related quality of life Effects are less convincing when the meta-analyses were restricted to those RCTs that specifically explored the role of IMT as an adjunct to a program of exercise training gains were reported in inspiratory muscle strength, but not exercise tolerance, symptoms, or health-related quality of life Todays approach support its use in those people with marked inspiratory muscle weakness As little as 5 weeks of high-intensity IMT is capable of inducing changes in respiratory muscle morphology It seems reasonable to offer IMT to those people who continue to experience intractable dyspnea despite completion of a comprehensive pulmonary rehabilitation program
116 NON-INVASIVE VENTILATION Counter the effects of dynamic hyperinflation on respiratory muscle function Aim of NIV during exercise is to unload the respiratory muscles, thus reducing the oxygen cost of breathing and delaying the onset of intolerable dyspnea Within a single exercise session, NIV has been shown to decrease inspiratory muscle effort, increase inspiratory and expiratory flows, increase minute ventilation, and improve gas exchange compared with exercise without ventilatory support Review + meta-analysis including 7 trials of NIV vs unassisted breathing during cycling or walking in COPD NIV increased endurance time by an average of 3.3 minutes (55%)
117 NIV during lower limb resistance exercise has been shown to delay the onset of quadriceps fatigue Increase in blood flow to the muscles? possibly as a result of redirection of the available cardiac output from respiratory muscles that are unloaded under NIV Use of NIV during an entire 6 wk 8 wk exercise training program has consistently been associated with improved exercise outcomes in people with advanced COPD Use of NIV during an entire 6 wk 8 wk exercise training program has consistently been associated with improved exercise outcomes in people with advanced COPD
118 Compared with training on room air or oxygen, NIV-assisted training confers greater gains in: Maximum exercise performance Functional exercise capacity Endurance exercise capacity These benefits are likely related to training at a higher intensity No studies have evaluated whether these benefits persist over the longer-term Positive effects of NIV-assisted training are seen in RCTs in which the mean FEV1<40% predicted advanced disease Rehabilitation clinicians must have sufficient time and expertise in its implementation and titration, which is likely to limit this adjunct to a few centers
119 HELIOX/HELIUM-HYPEROXIA Heliox is formed when the nitrogen in air is replaced by helium, resulting in a gas that is 79% helium and 21% oxygen Helium has a lower density than nitrogen heliox has a density nearly 3 times lower than air significantly lower turbulence greater tendency toward laminar flow overall decrease in airway resistance
120 Single session of submaximalexercise in COPD Reduced dynamic hyperinflation Reduced respiratory muscle loading Increased exercise endurance time Less dyspnea Less leg fatigue Helium-hyperoxia (30% oxygen, 70% helium), may have even greater effects on dynamic hyperinflation and exercise endurance + additive and independent effects of each gas on the work of breathing Physiologic benefits of inhaling helium gas mixtures are most evident in those with more severe airflow obstruction Recent studies increased locomotor muscle oxygen delivery in people with moderate to severe COPD as a result of improvements in both systemic oxygen delivery + muscle blood flow

121 RCT s Benefits of breathing helium gas mixtures during exercise training may be apparent only if this intervention allows a higher training load to be applied
122 HELIOX/HELIUM-HYPEROXIA The complex nature of applying helium gas mixtures during exercise training + added expense and lack of conclusive clinical benefits, this therapy does not have a routine role in PR for COPD Further studies are required to establish whether heliox or helium-hyperoxia can augment the effects of exercise training in selected people with COPD, with sustained benefits after the training period
123 PARTITIONING EXERCISING MUSCLE MASS Ventilatory load imposed during exercise is related to the intensity and duration of exercise as well as the volume of exercising muscle mass During PR the ventilatory load is often reduced by reducing exercise intensity may compromise the effectiveness of the training program and reduce the likelihood of any physiologic adaptation in the exercising muscles 1999 partitioning the exercise muscle mass served to reduce the ventilatory load associated with exercise and, in turn, optimize the muscle-specific work rate
124 PARTITIONING EXERCISING MUSCLE MASS Compared with cycling using both legs, cycling at the same relevant intensity using only 1 leg increased constant power exercise time by a factor of studies that have compared the effect of completing a cyclebased exercise training program, using 2 legs simultaneously versus training each leg independently Both studies have shown that a protocol of 1-leg versus 2-leg cycling conferred greater gains in the peak power and peak rate of oxygen uptake measured on completion of the training program This approach seems to be readily translated into clinical practice

125
126 Broadening the Scope of Pulmonary Rehabilitation Traditionally provided to stable patients with moderate to severe COPD, typically in an outpatient setting Over the past decade - pulmonary rehabilitation for COPD provided in the peri-exacerbation period produces a strong signal in reduced hospital readmissions and even, perhaps, reduced mortality COPD patients with less severe disease also stand to benefit, perhaps to a similar degree as those with more advanced disease New and growing evidence now supports the effectiveness and often equivalent benefits of pulmonary rehabilitation in the non-copd respiratory patient Carefully structured pulmonary rehabilitation given in the home setting can result in reductions in dyspnea similar to those achieved in centerbased programs
127

128

129
130 כתובת לשאלות ד"ר רונן בר-יוסף מכון ריאות ילדים מרפאת פעילות גופנית ותזונה נכונה בילדים מכון לאורח חיים בריא בילדים בי"ח רות לילדים, רמב"ם טל' : פקס: סלולרי: מייל: r_bar-yoseph@rambam.health.gov.il
פעילות גופנית במחלות נשימה כרוניות
 פעילות גופנית במחלות נשימה כרוניות ד"ר רונן בר-יוסף מכון ריאות ילדים מרפאת פעילות גופנית ותזונה נכונה בי"ח רות לילדים, רמב"ם פברואר 2014 במסגרת "רפואת ספורט" - שנה א' SPORTS MEDICINE Physical activity
פעילות גופנית במחלות נשימה כרוניות ד"ר רונן בר-יוסף מכון ריאות ילדים מרפאת פעילות גופנית ותזונה נכונה בי"ח רות לילדים, רמב"ם פברואר 2014 במסגרת "רפואת ספורט" - שנה א' SPORTS MEDICINE Physical activity
Optimizing the Lung Transplant Candidate through Exercise Training. Lisa Wickerson BScPT, MSc Canadian Respiratory Conference April 25, 2014
 Optimizing the Lung Transplant Candidate through Exercise Training Lisa Wickerson BScPT, MSc Canadian Respiratory Conference April 25, 2014 Conflicts of Interest None to declare Learning Objectives At
Optimizing the Lung Transplant Candidate through Exercise Training Lisa Wickerson BScPT, MSc Canadian Respiratory Conference April 25, 2014 Conflicts of Interest None to declare Learning Objectives At
Pulmonary Rehabilitation in Chronic Lung Disease; Components and Organization. Prof. Dr. Müzeyyen Erk Cerrahpaşa Medical Faculty Chest Disease Dept.
 Pulmonary Rehabilitation in Chronic Lung Disease; Components and Organization Prof. Dr. Müzeyyen Erk Cerrahpaşa Medical Faculty Chest Disease Dept. Plan Chronic Respiratory Disease Definition Factors Contributing
Pulmonary Rehabilitation in Chronic Lung Disease; Components and Organization Prof. Dr. Müzeyyen Erk Cerrahpaşa Medical Faculty Chest Disease Dept. Plan Chronic Respiratory Disease Definition Factors Contributing
The Importance of Pulmonary Rehabilitation
 November 21, 2017 The Importance of Pulmonary Rehabilitation Presenter: George Pyrgos, MD 1 The importance of Pulmonary Rehabilitation George Pyrgos, MD Medical Director of the Angelos Lung Center at Medstar
November 21, 2017 The Importance of Pulmonary Rehabilitation Presenter: George Pyrgos, MD 1 The importance of Pulmonary Rehabilitation George Pyrgos, MD Medical Director of the Angelos Lung Center at Medstar
Lessons to be learned from cardiopulmonary rehabilitation
 REHABILITATION AFTER CRITICAL ILLNESS: Lessons to be learned from cardiopulmonary rehabilitation Rik Gosselink, PT, PhD, FERS Faculty of Kinesiology and Rehabilitation Sciences University Hospitals Leuven,
REHABILITATION AFTER CRITICAL ILLNESS: Lessons to be learned from cardiopulmonary rehabilitation Rik Gosselink, PT, PhD, FERS Faculty of Kinesiology and Rehabilitation Sciences University Hospitals Leuven,
Update on Pulmonary Rehabilitation Programme. HA Convention Dr. Wong WY, Ida Haven of Hope Hospital 8 May 2018
 Update on Pulmonary Rehabilitation Programme HA Convention Dr. Wong WY, Ida Haven of Hope Hospital 8 May 2018 Impacts of COPD to patients Increase dyspnoea Limitation of activity Decrease quality of life
Update on Pulmonary Rehabilitation Programme HA Convention Dr. Wong WY, Ida Haven of Hope Hospital 8 May 2018 Impacts of COPD to patients Increase dyspnoea Limitation of activity Decrease quality of life
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO
 OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO Subject Index ACE inhibitors, see Angiotensin-converting enzyme inhibitors Aging
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO Subject Index ACE inhibitors, see Angiotensin-converting enzyme inhibitors Aging
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
Common Chronic diseases An Evidence Base for Yoga Intervention in Advanced Years & at End of Life
 Common Chronic diseases An Evidence Base for Yoga Intervention in Advanced Years & at End of Life Coronary artery disease Arthritis Hypertension Diabetes mellitus Obesity 1 2 Taking it easy Contributes
Common Chronic diseases An Evidence Base for Yoga Intervention in Advanced Years & at End of Life Coronary artery disease Arthritis Hypertension Diabetes mellitus Obesity 1 2 Taking it easy Contributes
Pulmonary rehabilitation in severe COPD.
 Pulmonary rehabilitation in severe COPD daniel.langer@faber.kuleuven.be Content Rehabilitation (how) does it work? How to train the ventilatory limited patient? Chronic Obstructive Pulmonary Disease NHLBI/WHO
Pulmonary rehabilitation in severe COPD daniel.langer@faber.kuleuven.be Content Rehabilitation (how) does it work? How to train the ventilatory limited patient? Chronic Obstructive Pulmonary Disease NHLBI/WHO
Cardiac Rehabilitation Program for LVAD Patients. Dr Katherine Fan Consultant Cardiologist Grantham Hospital, Hong Kong SAR
 Cardiac Rehabilitation Program for LVAD Patients Dr Katherine Fan Consultant Cardiologist Grantham Hospital, Hong Kong SAR Left Ventricular Assist Devices (LVAD) Improved Survival Following LVAD Implantations
Cardiac Rehabilitation Program for LVAD Patients Dr Katherine Fan Consultant Cardiologist Grantham Hospital, Hong Kong SAR Left Ventricular Assist Devices (LVAD) Improved Survival Following LVAD Implantations
Chronic Obstructive Pulmonary Disease (COPD) is a systematic disease with
 is a systematic disease with") Chronic Obstructive Pulmonary Disease (COPD) is a systematic disease with considerable impact on several dimensions of daily life. Those that suffer from COPD can be submitted to rehabilitation programmes.
Chronic Obstructive Pulmonary Disease (COPD) is a systematic disease with considerable impact on several dimensions of daily life. Those that suffer from COPD can be submitted to rehabilitation programmes.
Treatment. Assessing the outcome of interventions Traditionally, the effects of interventions have been assessed by measuring changes in the FEV 1
 58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Outpatient Pulmonary Rehabilitation
 Outpatient Pulmonary Rehabilitation Policy Number: 8.03.05 Last Review: 7/2017 Origination: 7/1995 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for
Outpatient Pulmonary Rehabilitation Policy Number: 8.03.05 Last Review: 7/2017 Origination: 7/1995 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
Exercise Stress Testing: Cardiovascular or Respiratory Limitation?
 Exercise Stress Testing: Cardiovascular or Respiratory Limitation? Marshall B. Dunning III, Ph.D., M.S. Professor of Medicine & Physiology Medical College of Wisconsin What is exercise? Physical activity
Exercise Stress Testing: Cardiovascular or Respiratory Limitation? Marshall B. Dunning III, Ph.D., M.S. Professor of Medicine & Physiology Medical College of Wisconsin What is exercise? Physical activity
The Art and Science of Pulmonary Rehab. Pam Haines, RCP Cardiopulmonary Rehab Manager
 The Art and Science of Pulmonary Rehab Pam Haines, RCP Cardiopulmonary Rehab Manager ATS/ERS Statement on PR As defined by the 2013 ATS/ERS Statement on Pulmonary Rehabilitation, PR is a comprehensive
The Art and Science of Pulmonary Rehab Pam Haines, RCP Cardiopulmonary Rehab Manager ATS/ERS Statement on PR As defined by the 2013 ATS/ERS Statement on Pulmonary Rehabilitation, PR is a comprehensive
Anti-tussivestussives
 PULMONARY REHABILITATION IN COPD WHAT DO WE OFFER ROUTINELY? Treatment of exacerbation Treatment of heart failure Treatment of infection Maintainance pharmacotherapy Domicillary oxygen Help for smoking
PULMONARY REHABILITATION IN COPD WHAT DO WE OFFER ROUTINELY? Treatment of exacerbation Treatment of heart failure Treatment of infection Maintainance pharmacotherapy Domicillary oxygen Help for smoking
Outpatient Pulmonary Rehabilitation
 Outpatient Pulmonary Rehabilitation Policy Number: 8.03.05 Last Review: 7/2018 Origination: 7/1995 Next Review: 7/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for
Outpatient Pulmonary Rehabilitation Policy Number: 8.03.05 Last Review: 7/2018 Origination: 7/1995 Next Review: 7/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for
PULMONARY REHABILITATION Current Evidence and Recommendations
 PULMONARY REHABILITATION Current Evidence and Recommendations Overview Introduction to Pulmonary Rehabilitation Pathophysiolgy of Exercise Limitation Exercise training Current evidence for COPD Current
PULMONARY REHABILITATION Current Evidence and Recommendations Overview Introduction to Pulmonary Rehabilitation Pathophysiolgy of Exercise Limitation Exercise training Current evidence for COPD Current
Clinical pulmonary physiology. How to report lung function tests
 Clinical pulmonary physiology or How to report lung function tests Lung function testing A brief history Why measure? What can you measure? Interpretation/ reporting Examples and case histories Exercise
Clinical pulmonary physiology or How to report lung function tests Lung function testing A brief history Why measure? What can you measure? Interpretation/ reporting Examples and case histories Exercise
Applied Exercise and Sport Physiology, with Labs, 4e
 Applied Exercise and Sport Physiology, with Labs, 4e hhpcommunities.com/exercisephysiology/chapter-10-aerobic-exercise-prescriptions-for-public-health-cardiorespiratory-fitness-and-athletics/chap Chapter
Applied Exercise and Sport Physiology, with Labs, 4e hhpcommunities.com/exercisephysiology/chapter-10-aerobic-exercise-prescriptions-for-public-health-cardiorespiratory-fitness-and-athletics/chap Chapter
Chronic inflammation of the airways Hyperactive bronchi Shortness of breath Tightness in chest Coughing Wheezing
 Chronic inflammation of the airways Hyperactive bronchi Shortness of breath Tightness in chest Coughing Wheezing Components of the respiratory system Nasal cavity Pharynx Trachea Bronchi Bronchioles Lungs
Chronic inflammation of the airways Hyperactive bronchi Shortness of breath Tightness in chest Coughing Wheezing Components of the respiratory system Nasal cavity Pharynx Trachea Bronchi Bronchioles Lungs
Cardiopulmonary Physical Therapy. Haneul Lee, DSc, PT
 Cardiopulmonary Physical Therapy Haneul Lee, DSc, PT A comprehensive pulmonary rehabilitation program should incorporate the following components : Patient assessment and goal-setting Exercise and functional
Cardiopulmonary Physical Therapy Haneul Lee, DSc, PT A comprehensive pulmonary rehabilitation program should incorporate the following components : Patient assessment and goal-setting Exercise and functional
호흡재활치료 울산의대서울아산병원 호흡기내과 이상도
 호흡재활치료 울산의대서울아산병원 호흡기내과 이상도 Systemic (Extrapulmonary) effects in COPD Skeletal muscle dysfunction Osteoporosis Weight loss Sexual dysfunction Cardiovascular diseases (Gross et al., Curr Opin Pulm Med 2001;7:84)
호흡재활치료 울산의대서울아산병원 호흡기내과 이상도 Systemic (Extrapulmonary) effects in COPD Skeletal muscle dysfunction Osteoporosis Weight loss Sexual dysfunction Cardiovascular diseases (Gross et al., Curr Opin Pulm Med 2001;7:84)
Prapaporn Pornsuriyasak, M.D. Pulmonary and Critical Care Medicine Ramathibodi Hospital
 Prapaporn Pornsuriyasak, M.D. Pulmonary and Critical Care Medicine Ramathibodi Hospital Only 20-30% of patients with lung cancer are potential candidates for lung resection Poor lung function alone ruled
Prapaporn Pornsuriyasak, M.D. Pulmonary and Critical Care Medicine Ramathibodi Hospital Only 20-30% of patients with lung cancer are potential candidates for lung resection Poor lung function alone ruled
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Commissioning for Better Outcomes in COPD
 Commissioning for Better Outcomes in COPD Dr Matt Kearney Primary Care & Public Health Advisor Respiratory Programme, Department of Health General Practitioner, Runcorn November 2011 What are the Commissioning
Commissioning for Better Outcomes in COPD Dr Matt Kearney Primary Care & Public Health Advisor Respiratory Programme, Department of Health General Practitioner, Runcorn November 2011 What are the Commissioning
CLINICAL USE CASES FOR RMT
 1 of 5 CLINICAL USE CASES FOR RMT USE CASE: WEANING FROM MECHANICAL VENTILATOR Benefits: Quicker time to ventilator liberation and trach decannulation A majority of LTAC patients are hard to wean from
1 of 5 CLINICAL USE CASES FOR RMT USE CASE: WEANING FROM MECHANICAL VENTILATOR Benefits: Quicker time to ventilator liberation and trach decannulation A majority of LTAC patients are hard to wean from
CARE OF THE ADULT COPD PATIENT
 CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
PHYSICAL FITNESS 1.- ENDURANCE TRAINING SYSTEMS
 PHYSICAL FITNESS 1.- ENDURANCE TRAINING SYSTEMS 1.1.- TYPES Last year we learnt that there are two types, depending on the intensity of the exertion: this intensity depends on whether the oxygen for the
PHYSICAL FITNESS 1.- ENDURANCE TRAINING SYSTEMS 1.1.- TYPES Last year we learnt that there are two types, depending on the intensity of the exertion: this intensity depends on whether the oxygen for the
Mellen Center Approaches Exercise in MS
 Mellen Center Approaches Exercise in MS Framework: Physical exercise is generally recommended to promote fitness and wellness in individuals with or without chronic health conditions. Implementing and
Mellen Center Approaches Exercise in MS Framework: Physical exercise is generally recommended to promote fitness and wellness in individuals with or without chronic health conditions. Implementing and
Exercise for Health and Fitness
 Exercise for Health and Fitness Chapter 13 1 Figure 13.1 Current levels of physical activity among American adults 2 What is Physical Fitness? Definition: Five components of Physical Fitness: 3 Components
Exercise for Health and Fitness Chapter 13 1 Figure 13.1 Current levels of physical activity among American adults 2 What is Physical Fitness? Definition: Five components of Physical Fitness: 3 Components
Exercise Prescription Certificate Course
 Exercise Prescription Certificate Course Session 2: Principles and Frameworks for Exercise Prescription Dr. Raymond CHAN Hoi-fai MBChB (DUNDEE), MSc Sports Medicine (Glasg), MScSMHS(CUHK), MSpMed (New
Exercise Prescription Certificate Course Session 2: Principles and Frameworks for Exercise Prescription Dr. Raymond CHAN Hoi-fai MBChB (DUNDEE), MSc Sports Medicine (Glasg), MScSMHS(CUHK), MSpMed (New
Basics of Cardiopulmonary Exercise Test Interpretation. Robert Kempainen, MD Hennepin County Medical Center
 Basics of Cardiopulmonary Exercise Test Interpretation Robert Kempainen, MD Hennepin County Medical Center None Conflicts of Interest Objectives Explain what normally limits exercise Summarize basic protocol
Basics of Cardiopulmonary Exercise Test Interpretation Robert Kempainen, MD Hennepin County Medical Center None Conflicts of Interest Objectives Explain what normally limits exercise Summarize basic protocol
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
Advanced Concepts of Personal Training Study Guide Answer Key
 Advanced Concepts of Personal Training Study Guide Answer Key Lesson 22 Working with Special Populations LESSON TWENTY TWO Lesson Twenty Two Working with Special Populations WORKING WITH SPECIAL POPULATIONS
Advanced Concepts of Personal Training Study Guide Answer Key Lesson 22 Working with Special Populations LESSON TWENTY TWO Lesson Twenty Two Working with Special Populations WORKING WITH SPECIAL POPULATIONS
Performance Enhancement. Cardiovascular/Respiratory Systems and Athletic Performance
 Performance Enhancement Cardiovascular/Respiratory Systems and Athletic Performance Functions of the Cardiovascular System Deliver oxygen & nutrients to body tissues Carry wastes from the cells Anatomy
Performance Enhancement Cardiovascular/Respiratory Systems and Athletic Performance Functions of the Cardiovascular System Deliver oxygen & nutrients to body tissues Carry wastes from the cells Anatomy
Cardiorespiratory Physiology
 5 Cardiorespiratory Training In this chapter you will learn about: Cardiorespiratory activities make up the bulk of the physical activities in Levels 1 and 2 of the Physical Activity Pyramid (Chapter 4,
5 Cardiorespiratory Training In this chapter you will learn about: Cardiorespiratory activities make up the bulk of the physical activities in Levels 1 and 2 of the Physical Activity Pyramid (Chapter 4,
SHS FITNESS ACROSS THE P.E. CURRICULUM
 SHS FITNESS ACROSS THE P.E. CURRICULUM Five Health-Related Fitness components: Flexibility the ability to move a joint through a full range of motion A regular program of stretching may incorporate dynamic
SHS FITNESS ACROSS THE P.E. CURRICULUM Five Health-Related Fitness components: Flexibility the ability to move a joint through a full range of motion A regular program of stretching may incorporate dynamic
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Pulmonary Rehabilitation in COPD-An Important Non-pharmacological Treatment
 122 Review Article Pulmonary Rehabilitation in COPD-An Important Non-pharmacological Treatment Department of Adult Nursing, Maharajgunj Nursing Campus, Institute of Medicine, Tribhuvan University, Kathmandu,
122 Review Article Pulmonary Rehabilitation in COPD-An Important Non-pharmacological Treatment Department of Adult Nursing, Maharajgunj Nursing Campus, Institute of Medicine, Tribhuvan University, Kathmandu,
A Place For Airway Clearance Therapy In Today s Healthcare Environment
 A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
Mobilization and Exercise Prescription
 1 Clinicians can use this job aid as a tool to guide them through mobilization and exercise prescription with patients who have cardiopulmonary conditions. Mobilization and Exercise Prescription Therapy
1 Clinicians can use this job aid as a tool to guide them through mobilization and exercise prescription with patients who have cardiopulmonary conditions. Mobilization and Exercise Prescription Therapy
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Exercise Progression for the Cardiac, Pulmonary & PAD Patient
 Exercise Progression for the Cardiac, Pulmonary & PAD Patient Thomas P. Mahady MS CSCS CCRP Hackensack University Medical Center Hackensack Meridian Health Learning Objectives The Art of Exercise Prescription.
Exercise Progression for the Cardiac, Pulmonary & PAD Patient Thomas P. Mahady MS CSCS CCRP Hackensack University Medical Center Hackensack Meridian Health Learning Objectives The Art of Exercise Prescription.
Lecture 6 Fitness Fitness 1. What is Fitness? 2. Cardiorespiratory Fitness 3. Muscular Fitness 4. Flexibility 5. Body Composition
 Lecture 6 Fitness 1 Fitness 1. What is Fitness? 2. Cardiorespiratory Fitness 3. Muscular Fitness 4. Flexibility 5. Body Composition 2 1 Americans (on average) are not a healthy bunch 3 Sitting is the new
Lecture 6 Fitness 1 Fitness 1. What is Fitness? 2. Cardiorespiratory Fitness 3. Muscular Fitness 4. Flexibility 5. Body Composition 2 1 Americans (on average) are not a healthy bunch 3 Sitting is the new
Pulmonary Rehabilitation Focusing on Rehabilitative Exercise Prof. Richard Casaburi
 Pulmonary Rehabilitation 1 Rehabilitation Clinical Trials Center Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center Torrance, California, USA Historical perspective on rehabilitative
Pulmonary Rehabilitation 1 Rehabilitation Clinical Trials Center Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center Torrance, California, USA Historical perspective on rehabilitative
Cardiopulmonary Exercise Testing in Cystic Fibrosis
 Cardiopulmonary Exercise Testing in Cystic Fibrosis Owen Tomlinson MSc, AFHEA Children s Health & Exercise Research Centre University of Exeter James Shelley MSc Physical Activity Exchange Liverpool John
Cardiopulmonary Exercise Testing in Cystic Fibrosis Owen Tomlinson MSc, AFHEA Children s Health & Exercise Research Centre University of Exeter James Shelley MSc Physical Activity Exchange Liverpool John
Steven S. Saliterman, MD, FACP
 Ashley Wagner, Sochi 2014 www.gotceleb.com Steven S. Saliterman, MD, FACP Adjunct Professor Department of Biomedical Engineering, University of Minnesota http://saliterman.umn.edu/ Aerobic (Oxidative Phosphorylation)
Ashley Wagner, Sochi 2014 www.gotceleb.com Steven S. Saliterman, MD, FACP Adjunct Professor Department of Biomedical Engineering, University of Minnesota http://saliterman.umn.edu/ Aerobic (Oxidative Phosphorylation)
leisure or sport skills living activities and other activities with vigor Ø Physical fitness: ability of the body to respond to physical demands
 LEARNING OBJECTIVES Ø Discuss benefits and guidelines of physical activity and exercise Ø Explain the components of health-related fitness Ø Explain how to improve health through moderate physical activity
LEARNING OBJECTIVES Ø Discuss benefits and guidelines of physical activity and exercise Ø Explain the components of health-related fitness Ø Explain how to improve health through moderate physical activity
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
Chapter 21 Training for Anaerobic and Aerobic Power
 Section 06: Exercise Training to Improve Performance Chapter 21 Training for Anaerobic and Aerobic Power Chapter 22 Muscular Strength: Training Muscles to Become Stronger Chapter 23 Special Aids to Exercise
Section 06: Exercise Training to Improve Performance Chapter 21 Training for Anaerobic and Aerobic Power Chapter 22 Muscular Strength: Training Muscles to Become Stronger Chapter 23 Special Aids to Exercise
Chronic Obstructive Pulmonary Disease (COPD) Copyright 2014 by Mosby, an imprint of Elsevier Inc.
 Copyright 2014 by Mosby, an imprint of Elsevier Inc.") Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
The addition of non-invasive ventilation during exercise training in COPD patients. Enrico Clini and Michelle Chatwin
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Fariba Rezaeetalab Associate Professor,Pulmonologist
 Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Strength and conditioning? Chapter 4 Training Techniques. Weight gain (24yr, 73kg, 177cm, takes 18% protein) Guidelines.
 Guidelines.") Strength and conditioning? Chapter 4 Training Techniques Minimise the probability of injury Maximise performance Athletic Training Spring 2014 Jihong Park Guidelines Safety: environment, technique, nutrition
Strength and conditioning? Chapter 4 Training Techniques Minimise the probability of injury Maximise performance Athletic Training Spring 2014 Jihong Park Guidelines Safety: environment, technique, nutrition
Fatigue in COPD. Dr. Jan Vercoulen, Clinical Psychologist. Dpt. Medical Psychology Radboud University Nijmegen Medical Center
 Fatigue in COPD Dr. Jan Vercoulen, Clinical Psychologist Dpt. Medical Psychology Radboud University Nijmegen Medical Center Definition COPD GOLD, 2016 Chronic Obstructive Pulmonary Disease = common preventable
Fatigue in COPD Dr. Jan Vercoulen, Clinical Psychologist Dpt. Medical Psychology Radboud University Nijmegen Medical Center Definition COPD GOLD, 2016 Chronic Obstructive Pulmonary Disease = common preventable
The Value of Exercise in the Cystic Fibrosis Clinic. Dr Patrick J Oades
 The Value of Exercise in the Cystic Fibrosis Clinic Dr Patrick J Oades WHO Global recommendations for physical activity and health 2010. Geneva: WHO Library Cataloguing-in-Publication Data. [ISBN: 978
The Value of Exercise in the Cystic Fibrosis Clinic Dr Patrick J Oades WHO Global recommendations for physical activity and health 2010. Geneva: WHO Library Cataloguing-in-Publication Data. [ISBN: 978
Fitness and You. What is Physical Fitness? 3/10/ health related components of physical fitness
 Fitness and You What is Physical Fitness? True fitness is maintaining recommended levels of activity and proper nutrition to allow achievement of fitness standards in ALL 5 COMPONENTS OF FITNESS. 5 health
Fitness and You What is Physical Fitness? True fitness is maintaining recommended levels of activity and proper nutrition to allow achievement of fitness standards in ALL 5 COMPONENTS OF FITNESS. 5 health
LABETTE COMMUNITY COLLEGE BRIEF SYLLABUS. Please check with the LCC bookstore for the required texts for this class.
 LABETTE COMMUNITY COLLEGE BRIEF SYLLABUS SPECIAL NOTE: This brief syllabus is not intended to be a legal contract. A full syllabus will be distributed to students at the first class session. TEXT AND SUPPLEMENTARY
LABETTE COMMUNITY COLLEGE BRIEF SYLLABUS SPECIAL NOTE: This brief syllabus is not intended to be a legal contract. A full syllabus will be distributed to students at the first class session. TEXT AND SUPPLEMENTARY
Physical activity guidelines To the Minister of Health, Welfare and Sport No. 2017/08e, The Hague, August 22, 2017
 Physical activity guidelines 2017 To the Minister of Health, Welfare and Sport No. 2017/08e, The Hague, August 22, 2017 Contents Physical activity guidelines 2017 page 2 of 45 contents Executive summary
Physical activity guidelines 2017 To the Minister of Health, Welfare and Sport No. 2017/08e, The Hague, August 22, 2017 Contents Physical activity guidelines 2017 page 2 of 45 contents Executive summary
What is Physical Fitness?
 What is Physical Fitness? The Body Systems ability to work together efficiently Daily activities require no effort Have the energy to respond in an emergency Can enjoy leisure activities Both Health and
What is Physical Fitness? The Body Systems ability to work together efficiently Daily activities require no effort Have the energy to respond in an emergency Can enjoy leisure activities Both Health and
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
FOLLOW-UP MEDICAL CARE OF SERVICE MEMBERS AND VETERANS CARDIOPULMONARY EXERCISE TESTING
 Cardiopulmonary Exercise Testing Chapter 13 FOLLOW-UP MEDICAL CARE OF SERVICE MEMBERS AND VETERANS CARDIOPULMONARY EXERCISE TESTING WILLIAM ESCHENBACHER, MD* INTRODUCTION AEROBIC METABOLISM ANAEROBIC METABOLISM
Cardiopulmonary Exercise Testing Chapter 13 FOLLOW-UP MEDICAL CARE OF SERVICE MEMBERS AND VETERANS CARDIOPULMONARY EXERCISE TESTING WILLIAM ESCHENBACHER, MD* INTRODUCTION AEROBIC METABOLISM ANAEROBIC METABOLISM
Lung Volume Reduction Surgery. February 2013
 Lung Volume Reduction Surgery February 2013 Presentation Outline Lung Volume Reduction Surgery (LVRS) Rationale & Historical Perspective NETT Results Current LVRS Process (from referral to surgery) Diagnostic
Lung Volume Reduction Surgery February 2013 Presentation Outline Lung Volume Reduction Surgery (LVRS) Rationale & Historical Perspective NETT Results Current LVRS Process (from referral to surgery) Diagnostic
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Concepts of Health and Fitness Physical Education Final Exam Review
 Concepts of Health and Fitness Physical Education Final Exam Review Benefits of Exercise 1. Lowers resting heart rate 2. Releases daily stress 3. Reduces risk of heart disease 4. Improves circulation and
Concepts of Health and Fitness Physical Education Final Exam Review Benefits of Exercise 1. Lowers resting heart rate 2. Releases daily stress 3. Reduces risk of heart disease 4. Improves circulation and
Alpha-1 Antitrypsin Deficiency Alpha-1 Lung Disease
 Alpha-1 Antitrypsin Deficiency Alpha-1 Lung Disease Chronic obstructive pulmonary disease (COPD) affects millions of people each year. Chronic means long term, obstructive means it is hard to get air in
Alpha-1 Antitrypsin Deficiency Alpha-1 Lung Disease Chronic obstructive pulmonary disease (COPD) affects millions of people each year. Chronic means long term, obstructive means it is hard to get air in
Cardiac & Pulmonary Rehab Individual Treatment Plan
 Initial Assessment Date: Re-Assessment Date: Re-Assessment Date: Follow-Up Discharge Date: Risk Assessment Risk Assessment Risk Assessment Risk Assessment BP SpO2 BP SpO2 BP SpO2 BP SpO2 HR Edema HR Edema
Initial Assessment Date: Re-Assessment Date: Re-Assessment Date: Follow-Up Discharge Date: Risk Assessment Risk Assessment Risk Assessment Risk Assessment BP SpO2 BP SpO2 BP SpO2 BP SpO2 HR Edema HR Edema
Chapter 12. Methods for Aerobic Training and Physiologic Responses
 Chapter 12 Methods for Aerobic Training and Physiologic Responses Aerobic Performance Purpose of training Improve performance General principles of physical conditioning Specificity Overload Aerobic Performance
Chapter 12 Methods for Aerobic Training and Physiologic Responses Aerobic Performance Purpose of training Improve performance General principles of physical conditioning Specificity Overload Aerobic Performance
Chapter 4. Muscular Strength and Endurance KIN 217 3/28/18 1
 Chapter 4 Muscular Strength and Endurance KIN 217 1 Functions of Muscle Tissues Functions: provide stability and postural tone, allow purposeful movement, heat production. Muscle mass constitutes: 40 to
Chapter 4 Muscular Strength and Endurance KIN 217 1 Functions of Muscle Tissues Functions: provide stability and postural tone, allow purposeful movement, heat production. Muscle mass constitutes: 40 to
They Can t Bury You while You re Still Moving: Update on Pulmonary Rehabilitation
 They Can t Bury You while You re Still Moving: Update on Pulmonary Rehabilitation Richard ZuWallack, MD Associate Chief, Pulmonary and Critical Care St. Francis Hospital, Hartford, CT Professor of Medicine
They Can t Bury You while You re Still Moving: Update on Pulmonary Rehabilitation Richard ZuWallack, MD Associate Chief, Pulmonary and Critical Care St. Francis Hospital, Hartford, CT Professor of Medicine
CRITICALLY APPRAISED PAPER (CAP)
") CRITICALLY APPRAISED PAPER (CAP) FOCUSED QUESTION In persons with chronic obstructive pulmonary disease (COPD), is a combination of exercise and activity-based breathing training more effective than a
CRITICALLY APPRAISED PAPER (CAP) FOCUSED QUESTION In persons with chronic obstructive pulmonary disease (COPD), is a combination of exercise and activity-based breathing training more effective than a
Resistance Training 101 Workshop
 UBC BodyWorks Fitness Centre Clinical Prevention Services Resistance Training 101 Workshop Presented By: Christina WM Sequeira, MKIN ACSM Certified Clinical Exercise Physiologist CSEP Exercise Physiologist
UBC BodyWorks Fitness Centre Clinical Prevention Services Resistance Training 101 Workshop Presented By: Christina WM Sequeira, MKIN ACSM Certified Clinical Exercise Physiologist CSEP Exercise Physiologist
Impact of Exercise on Patients with Diabetes Mellitus. Learning Objectives. Definitions Physical Activity and Health
 Impact of Exercise on Patients with Diabetes Mellitus Bret Goodpaster, Ph.D. Exercise Physiologist Assistant Professor of Medicine University of Pittsburgh Division of Endocrinology and Metabolism Learning
Impact of Exercise on Patients with Diabetes Mellitus Bret Goodpaster, Ph.D. Exercise Physiologist Assistant Professor of Medicine University of Pittsburgh Division of Endocrinology and Metabolism Learning
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Exercise: To do or not to do that is the question
 Exercise: To do or not to do that is the question What is exercise? To perform an activity to improve one s health Bodily or mental exertion, especially for the sake of training or improvement of health.
Exercise: To do or not to do that is the question What is exercise? To perform an activity to improve one s health Bodily or mental exertion, especially for the sake of training or improvement of health.
POLICIES AND PROCEDURE MANUAL
 POLICIES AND PROCEDURE MANUAL Policy: MP230 Section: Medical Benefit Policy Subject: Outpatient Pulmonary Rehabilitation I. Policy: Outpatient Pulmonary Rehabilitation II. Purpose/Objective: To provide
POLICIES AND PROCEDURE MANUAL Policy: MP230 Section: Medical Benefit Policy Subject: Outpatient Pulmonary Rehabilitation I. Policy: Outpatient Pulmonary Rehabilitation II. Purpose/Objective: To provide
Course Handouts & Disclosure
 COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
The Benefits Effects of Exercise for over 65s. Anna Haendel Physiotherapist
 The Benefits Effects of Exercise for over 65s Anna Haendel Physiotherapist Functional Capacity Objectives Describe the normal changes that occur with aging. How Physical Activity affects these changes
The Benefits Effects of Exercise for over 65s Anna Haendel Physiotherapist Functional Capacity Objectives Describe the normal changes that occur with aging. How Physical Activity affects these changes
University of Toronto Rotation Specific Objectives. cardiac rehabilitation
 University of Toronto Rotation Specific Objectives Cardiac Rehabilitation For this rotation, please FOCUS the evaluation on the following CanMEDs roles: 1) Medical Expert; 2) Collaborator; 3) Health Advocate
University of Toronto Rotation Specific Objectives Cardiac Rehabilitation For this rotation, please FOCUS the evaluation on the following CanMEDs roles: 1) Medical Expert; 2) Collaborator; 3) Health Advocate
Benefits of Exercise The Reality of How Much Is Enough. Center for Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital
 Benefits of Exercise The Reality of How Much Is Enough Center for Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital Physiological Effects of Lung Disease Oxidative Stress = Cumulative damage
Benefits of Exercise The Reality of How Much Is Enough Center for Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital Physiological Effects of Lung Disease Oxidative Stress = Cumulative damage
BURNOUT The Overtraining Syndrome in Swimming
 BURNOUT The Overtraining Syndrome in Swimming Dr Ralph Richards Introduction There are numerous terms associated with a state of poor or diminished sporting performance; burnout, staleness, chronic fatigue,
BURNOUT The Overtraining Syndrome in Swimming Dr Ralph Richards Introduction There are numerous terms associated with a state of poor or diminished sporting performance; burnout, staleness, chronic fatigue,
LEARNING OBJECTIVES FOR COPD EDUCATORS
 LEARNING OBJECTIVES FOR COPD EDUCATORS For further Information contact: INTERNATIONAL NETWORK FOR RESPIRATORY CARE 16851 Mount Wolfe Road Caledon, ON Canada L7E 3P6 Phone: 905 880-1092 Fax: 905 880-9733
LEARNING OBJECTIVES FOR COPD EDUCATORS For further Information contact: INTERNATIONAL NETWORK FOR RESPIRATORY CARE 16851 Mount Wolfe Road Caledon, ON Canada L7E 3P6 Phone: 905 880-1092 Fax: 905 880-9733
Exercise, Physical Therapy and Fall Prevention
 Exercise, Physical Therapy and Fall Prevention University of Davis Medical Center Rosy Chow Neuro Clinical Specialist Physical Therapist Outline of Talk Role of Physical Therapy in care of people with
Exercise, Physical Therapy and Fall Prevention University of Davis Medical Center Rosy Chow Neuro Clinical Specialist Physical Therapist Outline of Talk Role of Physical Therapy in care of people with
Role of Aerobic Exercise in Post-polio Syndrome. Dr. Jülide Öncü,MD İstanbul Sisli Etfal Teaching Hospital
 Role of Aerobic Exercise in Post-polio Syndrome Dr. Jülide Öncü,MD İstanbul Sisli Etfal Teaching Hospital julide.oncu@sislietfal.gov.tr Why is aerobic exercise important? Post-polio symptoms Impaired functional
Role of Aerobic Exercise in Post-polio Syndrome Dr. Jülide Öncü,MD İstanbul Sisli Etfal Teaching Hospital julide.oncu@sislietfal.gov.tr Why is aerobic exercise important? Post-polio symptoms Impaired functional
Anyone who smokes and/or has shortness of breath and sputum production could have COPD
 COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
Pathophysiology of COPD 건국대학교의학전문대학원
 Pathophysiology of COPD 건국대학교의학전문대학원 내과학교실 유광하 Rate per 100 0,000 population 550 500 450 400 350 300 250 200 150 100 50 0 Heart disease Cancer Stroke 1970 1974 1978 1982 1986 1990 1994 1998 2002 Year of
Pathophysiology of COPD 건국대학교의학전문대학원 내과학교실 유광하 Rate per 100 0,000 population 550 500 450 400 350 300 250 200 150 100 50 0 Heart disease Cancer Stroke 1970 1974 1978 1982 1986 1990 1994 1998 2002 Year of
What do pulmonary function tests tell you?
 Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
COPD Management in LTC: Presented By: Jessica Denney RRT
 COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
RESPIRATORY PHYSIOLOGY Pre-Lab Guide
 RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
PRESENTED BY BECKY BLAAUW OCT 2011
 PRESENTED BY BECKY BLAAUW OCT 2011 Introduction In 1990 top 5 causes of death and disease around the world: Lower Respiratory Tract Infections Diarrhea Conditions arising during pregnancy Major Depression
PRESENTED BY BECKY BLAAUW OCT 2011 Introduction In 1990 top 5 causes of death and disease around the world: Lower Respiratory Tract Infections Diarrhea Conditions arising during pregnancy Major Depression
Wellness: Concepts and Applications 8 th Edition Anspaugh, Hamrick, Rosato
 Wellness: Concepts and Applications 8 th Edition Anspaugh, Hamrick, Rosato Increasing Cardiorespiratory Endurance Chapter 3 Physical Fitness Physical Fitness Performance-related fitness Health-related
Wellness: Concepts and Applications 8 th Edition Anspaugh, Hamrick, Rosato Increasing Cardiorespiratory Endurance Chapter 3 Physical Fitness Physical Fitness Performance-related fitness Health-related
Interventional procedures guidance Published: 20 December 2017 nice.org.uk/guidance/ipg600
 Endobronchial valve insertion to reduce lung volume in emphysema Interventional procedures guidance Published: 20 December 2017 nice.org.uk/guidance/ipg600 Your responsibility This guidance represents
Endobronchial valve insertion to reduce lung volume in emphysema Interventional procedures guidance Published: 20 December 2017 nice.org.uk/guidance/ipg600 Your responsibility This guidance represents
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 CHRONIC OBSTRUCTIVE PULMONARY DISEASE DEFINITION Chronic obstructive pulmonary disease (COPD) is a common preventable and treatable disease characterized by airflow limitation that is usually progressive
CHRONIC OBSTRUCTIVE PULMONARY DISEASE DEFINITION Chronic obstructive pulmonary disease (COPD) is a common preventable and treatable disease characterized by airflow limitation that is usually progressive
CLINICAL PATHWAY. Acute Medicine. Chronic Obstructive Pulmonary Disease
 CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts